We are seeing examples of RPSFTM application in oncology trials (especially open-label randomized trials) and in rare disease clinical trials.
Hussain et al (2022) published a paper on NEJM "Survival with Olaparib in Metastatic Castration-Resistant Prostate Cancer". The results were from an open-label, phase 3 trial where patients were randomly assigned in 2:1 ratio to receive olaparib or physician's choice of enzalutamide or abiraterone plus prednisone as the control therapy. Patients in the control therapy group were allowed to be crossed over to olaparib after imaging-based disease progression criteria were met. Overall survival was analyzed using the naïve approach (intention-to-treat approach). Sensitivity analysis using the RPSFTM method was then performed to adjust for control patient crossover to olaparib. Kaplan-Meier plots for the observed data and for crossover-adjusted analysis were depicted below:

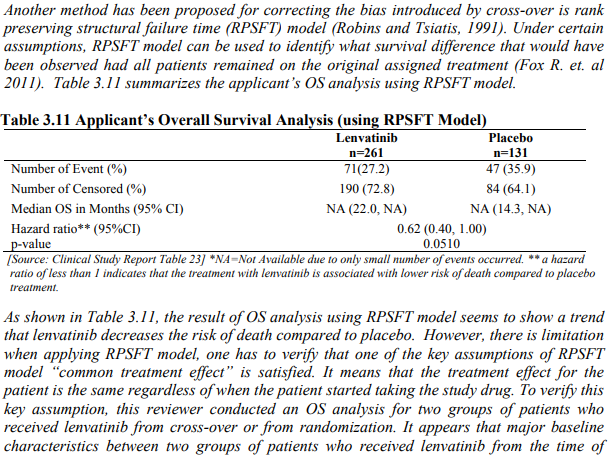
EISAI's Lenvatinib was approved for the treatment of patients with progressive, radioiodinerefractory differentiated thyroid cancer. The NDA approval was based on a pivotal study (Study 303). Study 303 is an international, double-blind, randomized 2:1, placebo-controlled, parallel-group, 2-arm trial. Patients would receive lenvatinib or placebo daily and could be treated until disease progression confirmd by IIR (RECIST v1.1) or unacceptable toxicity. The primary endpoint was progression-free survival with secondary endpoints of ORR and overall survival. Patients randomized to the placebo arm who had confirmed progression could choose to cross over and receive open-label lenvatinib. Overall survival was analyzed with the pooled data from the randomized portion of the study and the optional open-label extension phase. The effect of lenvatinib on overall survival was potentially confounded by the crossover of 83% of patients on the placebo arm to receive lenvatinib in the optional open-label (OOL) extension Phase.

Amylyx's RELYVRIO was approved by FDA for the treatment of ALS. The approval was based on a pivotal study (CENTAUR) and its open-label extension study (CENTAUR-OLE). The pivotal CENTAUR study was a randomized, placebo-controlled, double-blind, 24-weeks study in patients with ALS. Patients who completed 24-week randomized treatment were rolled over to an open-label extension study where all patients received the active drug. Patients in the active drug group in the randomized trial would continue with the active drug in the open-label extension study; patients in the placebo group in the randomized trial would switch or cross over to the active drug. To provide substantial evidence of the effectiveness of the active drug, the sponsor performed the analyses for long-term overall survival with the combined data from the randomized study and the open-label extension study. RPSFTM method was employed to handle the switch or crossover of the placebo patients in the randomized study to active drug in the OLE. Here is the description of the RPSFTM analysis from the briefing book for FDA Adcom.


The drug Uptravi was approved for the treatment of pulmonary arterial hypertension. The efficacy and safety were based on a pivotal study followed by an open-label extension study. The pivotal study was designed as an event-driven study where patients who had clinical worsening events would be rolled over to the open-label extension study. The placebo patients in the randomized study would switch or cross over the active drug in the open-label extension study. While the randomized study showed the treatment benefit in reducing the risk of clinical worsening events, there was an imbalance in the number of deaths (more death events in active drug group than the placebo group). The analyses for long-term overall survival with the combined data from the randomized study and the open-label extension study became necessary to mitigate the concern about the imbalance in the number of deaths observed in the randomized trial. RPSFTM method was employed to handle the switch or crossover of the placebo patients in the randomized study to the active drug in the OLE. EMA's assessment report described the RPSFTM analyses.

- R-package: https://cran.r-project.org/web/packages/rpsftm/vignettes/rpsftm_vignette.html
- Paper about R-package: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5858764/
- Danner and Sarkarto (2018) Implementing the Rank-Preserving Structural Failure Time Model in SAS® and R
- Paganoni et al (2022) Survival analyses from the CENTAUR trial in amyotrophic lateral sclerosis: Evaluating the impact of treatment crossover on outcomes
- Latimer et al (2016) Adjusting for treatment switching in the METRIC study shows further improved overall survival with trametinib compared with chemotherapy
- Latimer and Abrams (2014) NICE DSU Technical Support Document 16: Adjusting Survival Time Estimantes in the Presence of Treatment Switching
- Korhonen et al (2012) Correcting Overall Survival for the Impact of Crossover via a Rank-Preserving Structural Failure Time (RPSFT) Model in the RECORD-1 Trial of Everolimus in Metastatic Renal-cell Carcinoma
- White et al (1999) Randomization-based Methods for Correcting for Treatment Changes: Examples from the CONCORDE Trial
- Locke et al (2022) Axicabtagene Ciloleucel as Second-Line Therapy for Large B-Cell Lymphoma
- Bidard et al (2022) Switch to fulvestrant and palbociclib versus no switch inadvanced breast cancer with rising ESR1 mutation duringaromatase inhibitor and palbociclib therapy (PADA-1):a randomised, open-label, multicentre, phase 3 trial
- Turner et al (2018) Overall Survival with Palbociclib and Fulvestrant in Advanced Breast Cancer
- Zhu et al (2021) Final Overall Survival Efficacy Results of Ivosidenib for Patients With Advanced Cholangiocarcinoma With IDH1 Mutation
No comments:
Post a Comment