Platform trial is one type of Master protocol and refers to establishing the trial infrastructure and master protocol as a perpetuating effort, with drugs entering and leaving the platform.
Two prominent references for master protocols and platform trials are the following:
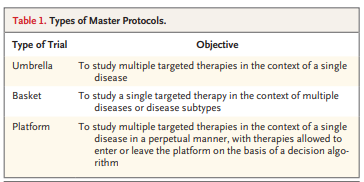
"Master Protocols to Study Multiple Therapies, Multiple Diseases, or Both" in 2017 by Woodcock and LaVange defines Master protocols include three type of trials: Umbrella, basket, and platform trials.
a master protocol is defined as a protocol designed with multiple substudies, which may have different objectives and involve coordinated efforts to evaluate one or more investigational drugs in one or more disease subtypes within the overall trial structure.
A master protocol may be used to conduct the trial or trials for exploratory purposes or to support a marketing application and can be structured to evaluate, in parallel, different drugs compared with their respective controls or to a single common control. The sponsor can design the master protocol with a fixed or adaptive design with the intent to modify the protocol to incorporate or terminate individual substudies within the master protocol.
Master protocols can include basket trial, umbrella trial, and platform trial and these trials can be schematically displayed as the following:
Basket trial



In a paper by Berry et al, "The Platform Trial An Efficient Strategy for Evaluating Multiple Treatments", the platform trial was compared to the traditional trial:

While platform trial has its challenges, we see the implementation trials in action, beyond the oncology trials. Here are examples of platform trials in areas other than the oncology trials. HEALEY ALS Platform Trial
The HEALEY ALS Platform Trial is a perpetual multi-center, multi-regimen clinical trial evaluating the safety and efficacy of investigational products for the treatment of ALS. This trial is designed as a perpetual platform trial. This means that there is a single Master Protocol dictating the conduct of the trial.
In this trial, multiple investigational products for ALS will be tested simultaneously or sequentially. Each investigational product will be tested in a regimen. Each regimen consists of a placebo-controlled trial, meaning that the active investigational product and matching placebo will be tested in each regimen.
PrecISE (Precision Interventions for Severe and/or Exacerbation-Prone Asthma) Network StudyThe study website is here: https://www.massgeneral.org/neurology/als/research/platform-trial
The study master protocol can be accessed here
Several testing drugs have been completed or graduated from the platform, please see the news releases
PrecISE is an adaptive platform trial under master protocol with common biomarker screening where drugs enter when available and discontinue based on futility analysis. According to clinicaltrials.gov, 5 novel interventions are currently listed as the testing drug for study: Medium Chain Triglycerides (MCT), Clazakizumab, Broncho-Vaxom, Imatinib Mesylate, Cavosonstat; each active will be tested against its own control.
the study design was described in the paper by Israel et al "PrecISE: Precision Medicine in Severe Asthma: An adaptive platform trial with biomarker ascertainment"REMAP-CAP: A Randomised, Embedded, Multi-factorial, Adaptive Platform Trial for Community-Acquired Pneumonia
ACTIV (NIH) Accelerating Covid-19 Therapeutic Interventions and VaccinesREMAP-CAP platform trial was originally designed for identifying the treatments for community-acquired pneumonia. After the Covid pandemic in 2020, REMAP-CAP has quickly implemented the Pandemic Appendix to the Core Protocol so that the platform can respond rapidly in the event of widespread disease resulting from the novel 2019 coronavirus (COVID-19).
Working in an unprecedented time frame, the Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) public–private partnership developed and launched 9 master protocols between 14 April 2020 and 31 May 2021 to allow for the coordinated and efficient evaluation of multiple investigational therapeutic agents for COVID-19. The ACTIV master protocols were designed with a portfolio approach to serve the following patient populations with COVID-19: mild to moderately ill outpatients, moderately ill inpatients, and critically ill inpatients.
The study design was described in the paper by LaVange et al "Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV): Designing Master Protocols for Evaluation of Candidate COVID-19 Therapeutics"RECOVER Clinical Trials - for Long Covid
Long COVID is defined as "a multifaceted disease that can affect nearly every organ system" and can manifest as new or worsening chronic health problems, including but not limited to heart disease, diabetes, kidney disease, hematologic issues, and mental and neurologic conditions. The signs, symptoms, and conditions continue or arise anew 4 weeks or more after the initial symptomatic or asymptomatic infection and may be relapsing and remitting.
NIH RECOVER trial is also using platform protocols/clinical trials to investigate treatments for long covid and master protocol is posted on the study website: https://trials.recovercovid.org/design. There will be multiple master protocols: RECOVER-VITAL, RECOVER-NEURO, RECOVER-AUTONOMIC (coming soon), RECOVER-SLEEP (coming soon) to investigate different
It is ironic that the RECOVER trial is started after NIH spent 2.5 years and $1 billion on long Covid research and failed to test meaningful long Covid treatments. See the article "Underwhelming’: NIH trials fail to test meaningful long Covid treatments — after 2.5 years and $1 billion "
Clinicaltrialsarena.com has an featured article "Platform trials: an opportunity for rare dystrophies or gene therapies?". The article discussed the possibility of platform trials in rare diseases and gene therapies. PaVeGT platform trial was listed:
PaVe-GT: Paving the Way for Rare Disease Gene Therapies
PaVe-GT will develop and test AAV-9, with a different gene for each indication, using a single master protocol. The NCATS-led Platform Vector Gene Therapy (PaVe-GT) pilot project seeks to increase the efficiency of clinical trial startup by using the same gene delivery system and manufacturing methods for multiple rare disease gene therapies. We will make program results and regulatory documents publicly available, with the intention of benefiting future gene therapy clinical trials for very rare diseases.
In a paper by Collignon (2022) "An Economic Perspective on Platform Trials—The Gift and the Curse", the following conclusion was made about the platform trial:
"...sharing a common control group in a platform trial can be viewed as a gift and a curse, and choosing whether to implement a platform trial or a more standard development program is complex since it is contingent on numerous factors that are disease and context dependent. To make such a decision, a clear framework needs to be implemented. Decision-making in the pharmaceutical industry is becoming increasingly more quantitative, and in practice, both development approaches would be compared according to a series of standard metrics, including(1) duration of the clinical program;(2) cost and expected reward of the clinical program;(3) flexibility of the clinical program (eg, reporting of the analyses corresponding to the different treatments while maintaining data and trial integrity, ability to add sites, and so forth); (4) probability of success for each treatment, for all treatments, or for at least 1 treatment, assuming all or some of the treatments have a certain efficacy;(5) probability of (multiple) false-positive findings (eg, achieving statistical significance) for each treatment or for at least 1 treatment, assuming all or some of the treatments are comparator-like; and(6) the extent to which a positive readout informs the success of potential subsequent trials and the ability to de-risk the next phase of development.Using these metrics, governance boards would then make their decisions on whether to progress developing a treatment according to a range of diverse considerations, such as portfolio opportunities and investment priorities."