Last Wednesday, The FDA in collaboration with the Duke-Margolis Center for Health Policy hosted a one-day virtual meeting focused on advancing premarket safety analytics. In the morning session, FDA officers discussed the FMQ (FDA Medical Query). In the afternoon session, FDA discussed the standardized presentation of the safety data including the tables and figures for adverse event data and laboratory data.
The FDA Medical Queries (FMQs) is a standardized approach to group preferred terms. Recognizing the limitation of the current analysis of adverse event data by preferred term, using FMQs can consolidate a medical condition with scattered preferred terms and be more likely to identify any signal of safety issues. The rationales for FDA's efforts in developing various FMQs are described in the slide below:


FMQs can be used to identify the safety signals that may be missed by using the conventional preferred term approach. When FMQs are adopted by the regulatory agency and the industry, FMQs (grouped term information) can be included in the ADVERSE REACTIONS Section of the Prescribing Information (or product label). The slide below illustrates a fictitious example of using FMQ term in the ADVERSE REACTIONS section of the product label. The AE table in the product label will include the mixture of the FMQ term (grouped term) and the MedDRA preferred terms.

A real example of FMQs in the product label can be the drug called Injectafer. The tables for adverse reactions included the mixture of the preferred terms and the grouped terms (based on FDA's FMQs).

With each version of the MedDRA dictionary, a set of available SMQs will be included. Included is also the document "Introductory Guide for Standardised MedDRAQueries (SMQs)".


It is true that SMQs have primarily been used in pharmacovigilance, not in premarket safety assessment. I have previously written a couple of articles about the SMQs:
FMQs were defined as the following:
FMQs can be used to identify the safety signals that may be missed by using the conventional preferred term approach. When FMQs are adopted by the regulatory agency and the industry, FMQs (grouped term information) can be included in the ADVERSE REACTIONS Section of the Prescribing Information (or product label). The slide below illustrates a fictitious example of using FMQ term in the ADVERSE REACTIONS section of the product label. The AE table in the product label will include the mixture of the FMQ term (grouped term) and the MedDRA preferred terms.
A real example of FMQs in the product label can be the drug called Injectafer. The tables for adverse reactions included the mixture of the preferred terms and the grouped terms (based on FDA's FMQs).
FMQ is exactly the same concept as the SMQ (standardized MedDRA query). The SMQ was defined as the following:
With each version of the MedDRA dictionary, a set of available SMQs will be included. Included is also the document "Introductory Guide for Standardised MedDRAQueries (SMQs)".
Both FMQ and SMQs included narrow terms and broad terms. However, the narrow terms are more commonly used in practice.
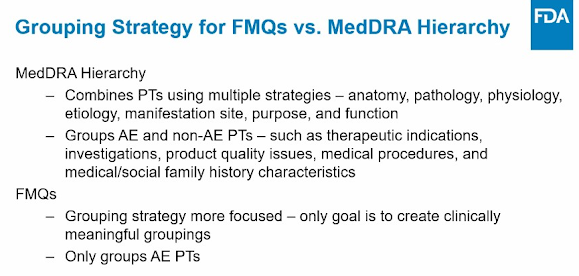
One natural question is: what is the difference between FMQ and SMQ? why can't we just use the SMQ? Here are a couple of slides indicating the differences between FMQ and SMQ. There are almost equal numbers of FMQs (104 FMQs for now) to SMQs (110 SMQs).
It is true that SMQs have primarily been used in pharmacovigilance, not in premarket safety assessment. I have previously written a couple of articles about the SMQs:
One drawback of FMQ is that it is developed by the US FDA and its use and application may be limited for market authorization applications in countries outside the US.
One thing for sure is that we will hear the term FMQ more often in the future and may see the request from FDA to present the grouped terms according to FMQs in the summary and analysis tables for AEs.
Further reading: